All published articles of this journal are available on ScienceDirect.

A Comparative Study between Melatonin and Midazolam as Premedication for Preoperative Anxiety in Patients Undergoing Cataract Surgery Under General Anesthesia: A Clinical Trial
Authors Info & Affiliations
Abstract
Introduction
Preoperative anxiety is a common concern among surgical patients and a key focus for anesthesiologists. Premedication, such as melatonin—an emerging option for sedation before cataract surgery—and midazolam, a routinely used benzodiazepine, play a vital role in managing anxiety and ensuring effective anesthetic care. This study aimed to compare the effects of melatonin and midazolam on the anxiety of cataract surgery candidates under general anesthesia.
Methods
This study included 40 patients scheduled for cataract surgery under general anesthesia at a surgical center in Birjand, Iran. Participants were randomly divided into two groups: one received 0.1 mg/kg oral melatonin, and the other received 70–80 µg/kg IV midazolam as premedication. Anesthesia was induced uniformly with fentanyl (1 µg/kg), propofol (2 mg/kg), and atracurium (0.5 mg/kg). Anxiety levels were assessed using the Beck Anxiety Inventory at two-time points: before premedication (baseline) and 1.5 hours after administration (30 minutes pre-surgery).
Results
There was no significant difference in the comparison of the average anxiety score after and before the premedication in the two investigated groups. The average anxiety score after the premedication in the midazolam group was not significantly different compared to before the premedication (P=0.817), but the average anxiety score in the melatonin group after the premedication was significantly reduced compared to before the premedication (P<0.001).
Discussion
Both melatonin and midazolam similarly reduced preoperative anxiety in cataract surgery patients, with melatonin potentially offering a safer profile. Further studies could explore its wider use as an alternative to benzodiazepines.
Conclusion
Melatonin may serve as a suitable alternative to midazolam for reducing preoperative anxiety. Given its better safety profile, further investigation of its broader applications is recommended.
1. BACKGROUND
Cataract is one of the main causes of visual impairment in the world and the main cause of blindness in 51% of cases of blindness worldwide [1]. Today, surgery is the treatment method for cataract recovery, which replaces the cloudy and opaque lens with an artificial transparent lens. Performing surgery is associated with anxiety and stress before and during the operation [2], and anxiety before surgery affects the psychological and physiological aspects of patients [3]. This anxiety leads to changes in the hemodynamics of patients [4]. A high level of anxiety increases the risk of death up to 3 times [5]. According to studies, 80% of patients admitted to the hospital suffer from anxiety and 71% of them do not receive any special nursing or medical care [6]. In a study by Khezri et al., it was reported that although most patients had negligible preoperative anxiety, some patients (14%) were found to have high levels of anxiety [4].
Anxiety affects various aspects of health and causes nausea and vomiting, urinary retention, restlessness, increased requests for painkillers, increased duration, decreased ability to fight infection, and delayed wound healing [7].
The main purpose of sedation in surgery is to prepare the patient to remain calm during the surgery [8]. Different drugs, such as propofol and benzodiazepines (midazolam), are used for sedation during surgery, which leads to impaired cooperation of patients before surgery [9]. Midazolam is commonly used as premedication in medical settings. Midazolam, a benzodiazepine, is effective in reducing anxiety and inducing sedation, making it useful for patients undergoing stressful procedures. However, it may cause side effects such as respiratory depression, especially in older adults or those with underlying health conditions. On the other hand, melatonin, a natural hormone, is known for its role in regulating sleep and has fewer side effects compared to midazolam [10]. Some studies have stated that melatonin is used as a new drug for sedation before cataract surgery [11]. Melatonin or N-acetyl methoxy tryptamine is a neurohormone produced by the pineal gland. However, the results of various studies on it are discussed [12]. Some other studies have stated that this drug, as a pre-operative anesthetic, causes sedation and reduces pre-operative anxiety without cognitive impairment, such as memory and recall impairment [13].
2. OBJECTIVES
Considering that the studies conducted on the effectiveness of melatonin were limited and various studies had suggested conducting studies on this drug, our aim in this study was to compare the effect of melatonin and midazolam on the level of anxiety in patients who were candidates for cataract surgery under general anesthesia.
3. METHOD
After obtaining the ethical approval with the code IR.BsUMS.REC.1400.324 from Research and Technology of Birjand University of Medical Sciences and registration in the trial center of this study to IRCT 20190618043934 N15, this study was conducted as a randomized controlled clinical trial. This study was conducted on 40 patients scheduled for cataract surgery under general anesthesia at the eye surgery department of Razi Hospital in Birjand, Iran. Inclusion criteria included informed consent to enter the study, ASA class 1 and 2, and exclusion criteria included drug addiction, non-cooperation with the study administrator, heart failure, uncontrolled blood pressure, anticoagulant use, use of antiepileptic drugs, immunosuppressive drugs, history of liver or kidney diseases, confusion, dementia, lack of verbal communication, chronic use of narcotics, treatment with barbiturates or antipsychotic drugs, allergies or body mass index below 18.5 or above 30.
The sample size was calculated based on Patel's study [9] in 2015 with 95% confidence and 80% power, and the number of 17 people in each group was obtained, which was considered to be about 20 people with a 20% chance of dropping out. Patients scheduled for surgery were randomly divided into two groups using random allocation software.
4. INTERVENTIONS
Group 1: Patients received melatonin tablets at a dose of 0.1 mg per kilogram one hour before the operation. Group 2: Patients received midazolam at a dose of 70-80 micrograms per kilogram intravenously one hour before the operation. All patients were induced with fentanyl at a dose of one microgram per kilogram, propofol at a dose of two milligrams per kilogram, and atracurium at a dose of 0.5 mg per kilogram. The level of anxiety was evaluated at two-time points: Before premedication administration (baseline) and half an hour before surgery (after premedication administration).
Anxiety levels were assessed using the Beck Anxiety Questionnaire. Beck's anxiety questionnaire had 21 questions that were scored in a four-part spectrum from 0 to 3, and each test item described one of the common symptoms of anxiety (mental, physical, panic). The total score ranged from 0 to 63. Checking the reliability and validity of Beck's anxiety scale in students using Cronbach's alpha test of 0.92 had been confirmed by Rafiei et al. Both patients and the evaluator (researcher) were blinded to the group allocation and the specific drug administered to eliminate bias in the assessment. In addition, this study was conducted based on the CONSORT checklist (Fig. 1).
After collecting the data, the information was entered into SPSS software and analyzed. The significance level was considered to be 0.05. Comparison of frequency distribution in terms of sex and average age was done by chi-square test. To analyze the data in different groups, if there was a normal distribution, the independent, paired t-test was used, and if there was no normal distribution, the Mann-Whitney, Wilcoxon, Friedman test, and the Chi-square test or Fisher's exact test at a significance level of 0.05 ≥ α was used.
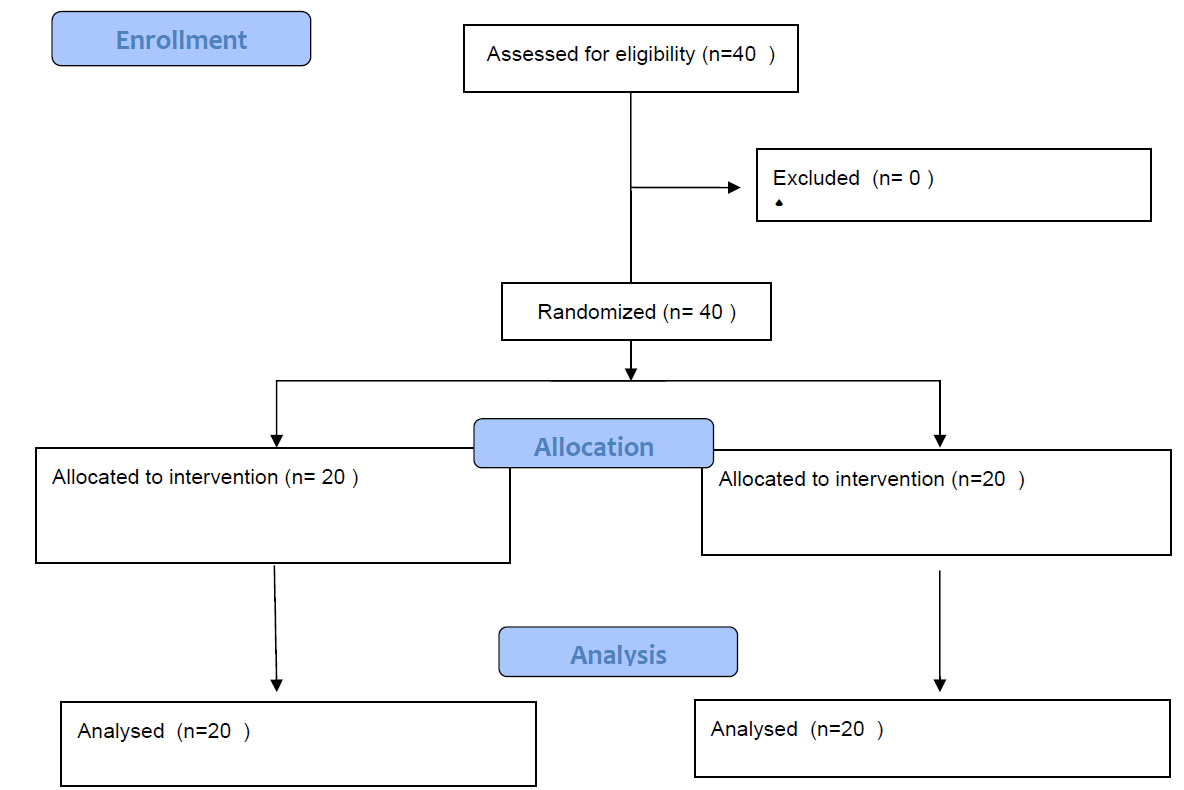
CONSORT flow diagram
5. RESULTS
In the present study, 40 patients were evaluated in two groups of 20 people. The distribution of sexual frequency, education level, place of residence and average age of patients in the two groups were not significantly different from each other (P>0.05). (Table 1)
According to the results of the present study, the t-test showed that the average anxiety score in the two groups did not have a significant difference before the premedication (P = 0.161). The average anxiety score after the premedication also did not show a significant difference between the two groups (P = 0.372). (Table 2) The results of the paired t-test showed that there was a significant difference in the average anxiety score before and after the premedication in the melatonin group (p=0.001), while no significant difference was observed in the midazolam group before and after the premedication (p=0.817) (Fig. 2).
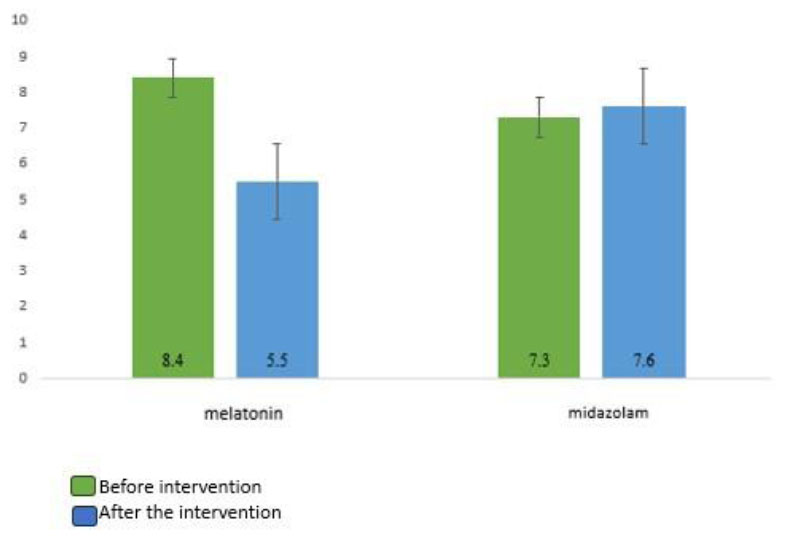
Comparison of the average anxiety scores of patients in two groups of midazolam and melatonin before and after the intervention.
| Variable | Midazolam | Melatonin | P Value |
|---|---|---|---|
| Age | - | - | - |
| Mean ± SD | 64.2±9.4 | 63.4±12.3 | 0.74 |
| Sex | - | - | - |
| Male | 10(50) | 11(55) | P=1.000 |
| Female | 10(50) | 9(45) | - |
|
Midazolam Mean ± SD (q3-q1) Median |
Melatonin Mean ± SD (q3-q1) Median |
Independent T-Test | |
|---|---|---|---|
| Before premedication | 7.3±3.8 (10-3.25)6 |
8.4±3.8 (12-5.25)8.5 |
T=1.428 P=0.161 |
| After premedication | 7.6±4.9 (10-4)6 |
5.5±4.3 (8-1)6.5 |
T=0.904 P=0.372 |
| Dependent T-Test | T=0.234 P=0.817 |
t-=4.28 p<0.001 |
- |
6. DISCUSSION
The study aimed to compare the effects of melatonin and midazolam on the anxiety levels of cataract surgery candidates under general anesthesia. The doses used in this study (5 mg of intravenous midazolam and 3 mg of oral melatonin) were chosen based on previous studies indicating that these doses are effective in reducing preoperative anxiety. The timing of anxiety assessment (1.5 hours after medication administration) was also chosen based on studies reporting the maximum anxiolytic effects of these medications during this timeframe [14].
The results revealed that while midazolam did not significantly reduce anxiety levels in patients, melatonin demonstrated a significant reduction in anxiety scores after administration (P < 0.001). This suggests that melatonin may be more effective than midazolam in alleviating preoperative anxiety in this patient population. In various studies, the effect of melatonin on reducing anxiety has been reported. In the study conducted by Camo et al., it was stated that the mean anxiety score in the melatonin group was lower than in the control group, which was consistent with our study [15]. In studies conducted by Acil et al., Samargandi et al., and Patel et al., it was reported that the mean anxiety score significantly decreased in the group receiving melatonin before surgery, which aligns with the findings of our study [9, 16, 17]. Similarly, research by Sury et al., Fairweather Kain et al., and Capuzzo et al. supports the effectiveness of melatonin in reducing preoperative anxiety [18, 19]. These consistent results across multiple studies highlight melatonin's potential as a reliable option for managing anxiety in surgical patients.
In Bheema Devanand's study, which examined oral midazolam with oral melatonin in children, the results showed that the onset and quality of anxiety were significantly better in the midazolam group than in the melatonin group, and in our study, the quality of anxiety was not investigated [14]. In Patel's study in 2023, which compared oral midazolam versus oral melatonin in patients aged 18 to 60 years before surgery, the anxiety score after taking the drug was not significant in the two groups, but the side effects of excessive sleepiness, nausea, vomiting, and visual impairment in the group Midazolam was more [9]. The results of the above two studies were not consistent with our study, which could be due to the type of patients selected or the difference in the method of taking midazolam in the study sample. On the other hand, in another study, it was also stated that the anti-anxiety and sleep-inducing effects of melatonin decrease in the elderly, and in other words, the elderly are resistant to melatonin, therefore, the anti-anxiety effects of melatonin decrease with age [7].
According to the results of various studies, melatonin demonstrates superior anti-anxiety effects compared to midazolam, which may be attributed to its interaction with the GABA system. Specifically, melatonin induces a significant, dose-dependent increase in GABA concentration within the central nervous system, thereby reducing anxiety levels. In the context of this study, the significant reduction in anxiety scores observed in the melatonin group (P < 0.001) further supports the hypothesis that melatonin's anxiolytic effects are mediated through GABAergic mechanisms, offering a potential advantage over midazolam for preoperative anxiety management [7, 20].
Studies have shown that melatonin exerts a calming effect by modulating gamma-aminobutyric acid (GABA<sub>A</sub>) receptors in the brain through its interaction with melatonin receptors (MT1 and MT2). The binding of melatonin to the MT1 receptor affects the GABAA receptor through the G protein pathway. This increased the binding of GABA to its receptor, which is similar to the action of other anesthetics such as propofol and benzodiazepines [21].
CONCLUSION
The results of the present study indicate that premedication with melatonin significantly reduces anxiety and provides better sedation compared to midazolam. To further validate these findings and explore the broader applications of melatonin, it is recommended to conduct similar studies investigating the effects of varying doses of melatonin on diverse patient populations. Additionally, future research should focus on examining the impact of different doses across various age groups to better understand the optimal use of melatonin for anxiety management in clinical settings.
LIMITATIONS OF THE STUDY
One limitation of this study is the measurement of anxiety levels 90 minutes after intravenous midazolam administration. Given that the anxiolytic effects of midazolam typically last for 1 to 2 hours, this measurement time may have fallen outside the peak effect window of the drug. Therefore, the results obtained may have been influenced by the timing of the assessment.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contributions to the manuscript as follows: MZ was responsible for conceptualization; ASY handled data collection; SS and MT prepared the draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| IR.BsUMS | = Institutional Review Board of Birjand University of Medical Sciences |
| IRCT | = Iranian Registry of Clinical Trials |
| ASA | = American Society of Anesthesiologists Physical Status Classification System |
| CONSORT | = Consolidated Standards of Reporting Trials |
| GABA | = Gamma-Aminobutyric Acid (γ-Aminobutyric Acid) |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval with the code IR.BUMS.REC.1400.324 from the esteemed Vice President of Research and Technology of Birjand University of Medical Sciences and registration in the trial center of this study to IRCT20190618043934N15 was obtained.
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIAL
The data sets used and/or analysed during this study are available from the corresponding author [M.T] upon request.
ACKNOWLEDGEMENTS
Declared none.